Nutritional Screening for Wound Care and Hyperbaric Oxygen Therapy
By Tiffany Hamm and Jeff Mize vai Multibriefs
This article originally appeared on WoundReference.
How important is nutritional assessment in hyperbaric oxygen therapy?
One of the keys to a successful patient outcome is assessing nutritional status. If the patient is malnourished, there is insufficient nutritional substrate from which to build new tissue to heal a wound. One out of three patients treated at hyperbaric services can be at risk of malnutrition.
The definition of a nutritional assessment in the National Coverage Determination NCD 20.29 for Hyperbaric Oxygen Therapy is vague. Although an assessment of nutritional status should be routinely performed on all patients seen in the outpatient wound clinic, the protocol is not well-defined. Many times, the patient’s nutritional evaluation and management is directed back to the primary care or referring physician.
NCD 20.29 states: "For diabetic wounds of the lower extremity, the use of HBO therapy is covered as adjunctive therapy only after there are no measurable signs of healing for at least 30 days of treatment with standard wound therapy and must be used in addition to standard wound care."
Standard wound care in patients with diabetic wounds includes optimization of nutritional status. Since the NCD requires this to be part of conservative care, documentation of nutritional status must be a part of the wound care and HBOT patient record. If this documentation is missing, the services may be denied post payment and funds recouped upon review by your Medicare Administrative Contractor (MAC).
How is optimization of nutritional status defined?
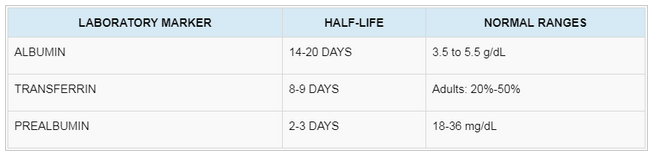
The requirements are not well defined by the NCD or any of the MACs (i.e., WPS, Novitas, Noridian). However, we suggest that laboratory documentation of nutritional status include: albumin, transferrin, and/or pre-albumin levels, with vitamin and trace mineral levels as clinically indicated. Also, since inflammation alters the levels of these markers, C-reactive protein may be of use in interpreting results.
Protein deficiencies are thought to contribute to poor healing rates. Proteins play the most important role throughout the entire wound-healing process. Cells of the immune system (e.g. lymphocytes, leukocytes, phagocytes, monocytes, and macrophages) are mainly comprised of proteins and are necessary to initiate a healthy inflammatory response in the healing process. An adequate supply with proteins is necessary for consistent wound healing. Because collagen is the protein that is produced mainly in the healing wound, a lack of protein decreases the synthesis of collagen and the production of fibroblasts.
According to the NCD 20.29, patients with DFUs require 30 days of optimization of all parameters. Using this timeframe, transferrin and prealbumin levels would show the greatest changes in the time period that is being reviewed (see table below).
Protein laboratory markers and their half-life and normal ranges
The initial intervention should consist of oral nutritional supplements such as high protein/high-calorie food items (e.g. eggs, meats, nuts, cheese, and prepackaged dietary supplements that include arginine, glutamine, and/or hydroxyl-methyl-buterate HMB).
Patients who are unable to adequately increase their protein consumption by simple oral nutritional supplements should be considered for tube feedings or parenteral nutritional support. Evaluation by a registered dietitian should be considered if there is an inadequate response to first-line oral interventions.
The body creates protein waste products when it ingests protein. In healthy kidneys, millions of nephrons filter waste products. If a patient has chronic kidney disease (CKD), the kidney loses the ability to remove protein waste. This waste builds up in the blood instead of being flushed out into the urine. Patients with CKD should consult their nephrologist or a registered dietician before increasing protein intake.
Patients who live with diabetes and experience delayed wound healing should balance optimization of nutrition with glycemic control. A multidisciplinary approach may be necessary to achieve clinical outcomes. Wound Centers should strive to develop a systematic approach to optimizing nutritional status in patients starting with the initial evaluation and reassessing at 30-day intervals.
Key takeaways
One of the keys to a successful patient outcome in HBOT is assessment of nutritional status. Malnutrition screening should be part of routine patient assessment in order to ensure patients receive timely nutritional intervention.
NCD 20.29 requires optimization of nutritional status to be part of conservative care thus documentation of nutritional status, plan and outcomes must be part of the wound care and HBOT patient record.
Tiffany Hamm, BSN, ACHRN, CWS is the co-founder and Chief Nursing Officer of WoundReference, Inc., a clinical and reimbursement decision support platform for wound care and hyperbaric clinicians. She is principal partner of Midwest Hyperbaric LLC, a hyperbaric and wound consultative service. Tiffany is also an Advanced Certified Hyperbaric Registered Nurse and Certified Wound Specialist with expertise in billing, coding and reimbursement specific to hyperbaric medicine and wound care services. UHMS Accreditation Surveyor. Tiffany received her primary and advanced hyperbaric training through National Baromedical Services in Columbia, South Carolina.
Jeff Mize, RRT, CHT, CWCA is co-founder and Chief Clinical Officer for Wound Reference, a clinical and reimbursement decision support platform for wound care and hyperbaric clinicians. He is principal partner with Midwest Hyperbaric LLC, a hyperbaric and wound consultative service. Jeff is a Registered Respiratory Therapist, a Certified Hyperbaric Technologist (CHT) by the National Board of Diving and Hyperbaric Medical Technology, and a Certified Wound Care Associate (CWCA) by the American Academy of Wound Management. After receiving primary hyperbaric training from National Baromedical Services, he trained as a UHMS Safety Director and is a UHMS Facility Accreditation Surveyor. He is the 2010 recipient of the Gurnee Award and the 2013 recipient of the Paul C. Baker Award for Hyperbaric Oxygen Safety Excellence. He has also served on the UHMS Board of Directors (2010-2015).
|



